

Understanding “late-term” abortions
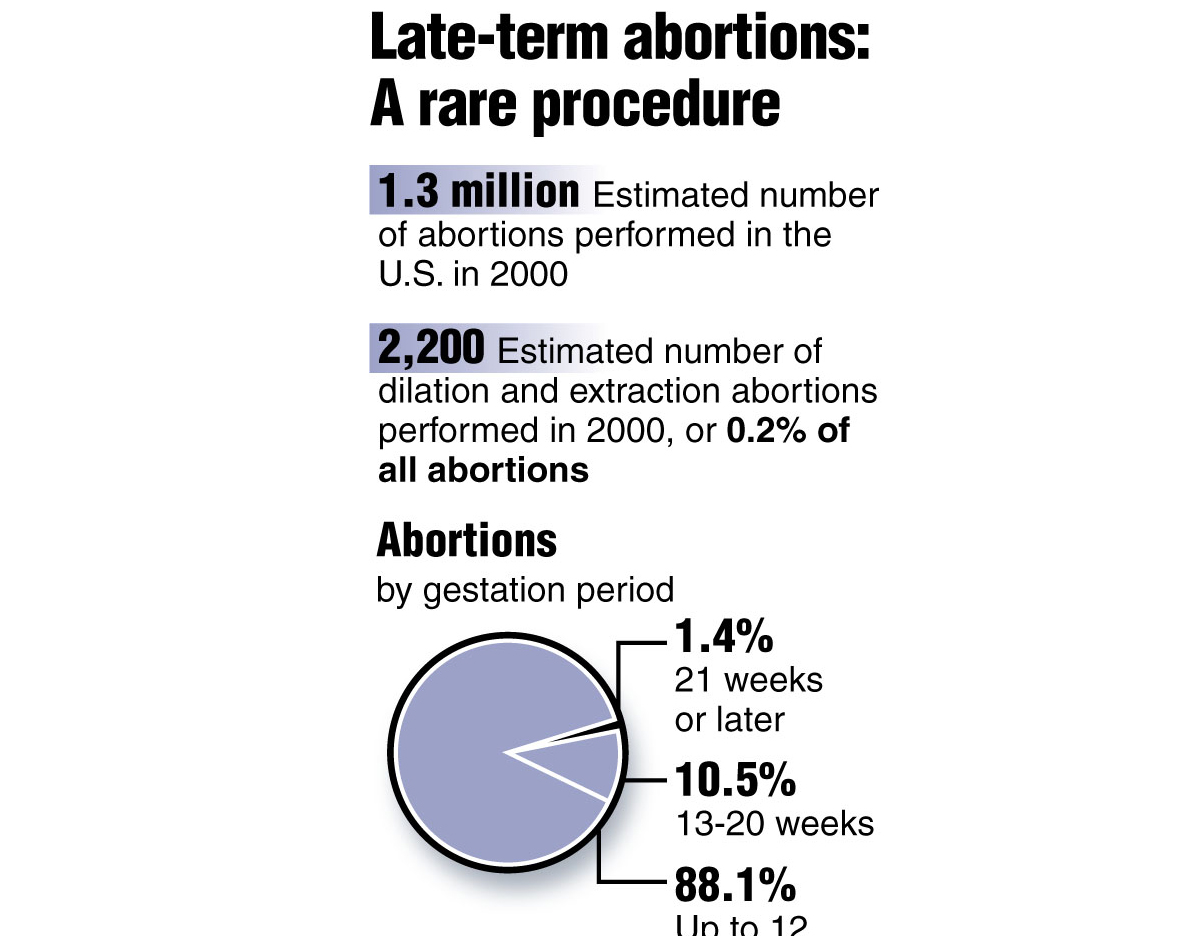
According to the Guttmacher Institute, dilation and extraction abortions comprised 0.2 percent of all abortions in the US, as of 2000.
Aug 31, 2017
First, let me tell you about my views on abortion and how they have evolved throughout my college career. When I walked onto campus as a freshman, I was 100 percent pro-life with no exceptions. My thought process was that “there is always adoption” and “pregnancy was a consequence of stupid decisions.”
However, I have always been open-minded and listened to the experiences of others. I heard people’s stories of rape and incest leading to an unwanted pregnancy and the trauma experienced carrying to term.
This changed my mind to believe that people should be able to have abortions before six weeks (when the heart beating can be heard for the first time). I believed this for a while, but then I heard personal stories of “late-term” abortions. I changed my mind again. As of now, I am 100 percent completely pro-choice and here’s why.
Most abortions occur in the beginning of a pregnancy. According to the Center for Disease Control and Prevention, 91.4 percent of abortions occur in the first trimester (less than 14 weeks into pregnancy). This is an overwhelming majority, and just 1.3 percent of abortions are performed at or after 21 weeks.
Why would someone have a “late-term” abortion? Well, basically it is because of health concerns that are often fatal. There are many fetal abnormalities that lead to death or extremely severe disabilities. Tay-Sachs disease, Zika infection, muscular development issues and brain defects are just a few examples.
According to Forbes, these serious health concerns usually cannot be identified until after the first 20 weeks. This means that the parents are expecting to carry a healthy baby to full-term, and they find out the devastating news that either themselves or the baby will probably die or have very serious health risks or suffer.
These are parents that have bought clothes, picked out names, started the nursery and shared their excitement with friends and family. Abortions that happen during the second or early third trimester are usually unwanted abortions, but are necessary to avoid horrific suffering or death to the person with the uterus and baby. As you can see, no parent wants a late-term abortion. It usually is their only option.
Now you may be thinking: So, a parent could decide the day before their due date to abort the baby? No, that is not a thing.
As Jen Gunter, an OB-GYN (obstetrics and gynecology) doctor trained in late-term abortions, said, “There is no such thing as a ninth month abortion.”
First, there are only two locations (Boulder, Colorado and Albuquerque, New Mexico) in the United States that perform late-term abortions; they will not perform the procedure on healthy babies, and they evaluate the ethics case by case. Feel free to check out their website and communicate with those doctors to confirm that they do not perform late-term abortions on everyone and that they actually turn people away.
What about that partial birth procedure? Well, that is not a medical term, and the term is not talking about late-term abortions at all. It is a rare procedure called dilation and extraction, which is performed nearly always when the fetus cannot survive outside the uterus and the parent’s life is in danger.
According to the Guttmacher Institute, 0.2 percent of all abortions use this very procedure. This is a type of procedure that can happen during the first trimester – not just late-term.
You may be thinking: Well, if we de-regulate abortion, the rates will just go up!
In reality, the exact opposite is true.
As the Albuquerque Journal stated, in 2010, New Mexico became the state with the fewest restrictions on abortion and since then, they have seen a 24 percent drop in abortions.
According to Forbes, New Mexico is following a national trend that reveals that states with the least restrictions on abortion also have the largest declines in the number of abortions performed.
There are many misconceptions about late-term abortions, and I hope I have cleared up some of the fallacies. I believe that the United States as a whole should allow parents and their doctors to decide what’s best for the health of the baby and the person with the uterus.
Each case is different.
Let’s follow in New Mexico’s steps and put our trust into women and doctors, knowing that they are making the best decisions.





